
Politics
Thousands Rally Behind Tidjane Thiam in Côte d’Ivoire
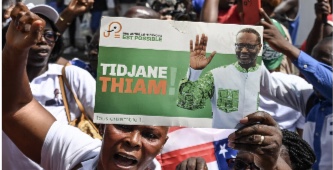
Thousands of Ivorians have taken to the streets to show their unwavering support for dissident opposition figure Tidjane Thiam, who was recently barred from contesting in the upcoming presidential election.
Despite the ban, Thiam’s supporters remain resolute in their backing, chanting “Thithi President!” and waving flags as they demand a more inclusive political process.
The controversy surrounding Thiam’s disqualification has sparked widespread criticism, with many accusing the government of manipulating the electoral process to silence opposition voices.
The Constitutional Council’s decision to exclude Thiam from the list of eligible candidates has been met with skepticism, with many questioning the legitimacy of the process.
To his supporters, Thiam represents a break from the old political elite and a hope for reform and transparency in governance.
They see him as a strong challenger to the ruling establishment, and his disqualification has only strengthened their resolve.
“We are not just rallying for a man; we are defending democracy,” one protester said. “They may ban him from the ballot, but they can’t ban his ideas.”
Although Thiam himself has called for calm and unity, urging his supporters to continue advocating for change.
In a press release, he emphasized the importance of respecting the people’s will and promoting reform and inclusivity in the political process.
“The future of Côte d’Ivoire does not lie in exclusion, but in unity, reform, and respect for the people’s will,” he stated.












Examining Nigeria’s Health System and Preventable Deaths, by Alabidun Shuaib AbdulRahman
My last week’s column, ‘The Agony of a Columnist,’ was written from a place I never expected to occupy. It was not an attempt at catharsis, nor was it designed to elicit sympathy. It was simply an account of what happened when a citizen encountered the Nigerian healthcare system at its most critical moment and found it wanting. The death of my eight-month-old daughter occurred within a public hospital that, on paper, appeared functional. What followed exposed a gap between appearance and capacity that deserves closer scrutiny rather than sentiment.
This week’s column is broader. It is about structure, policy, and outcomes. It is about what the data says and what lived experience confirms about the state of healthcare delivery in Nigeria, a system that reflects not only underperformance but failure at its most consequential moments.
Considering another recent case that captured national attention, that of Ifunanya Lucy Nwangene, a 25-year-old Abuja-based singer who was bitten by a cobra in her home. She sought emergency care immediately, moving from one health facility to another, and struggled to obtain antivenom and appropriate treatment before it was too late.
Accounts vary on the specifics, but the tragedy is indisputable. Her death, amid circumstances that could have been preventable, echoes the avoidable loss of my own child and reflects the same systemic weaknesses that place ordinary citizens at risk every day. Reports indicate that approximately half of Nigerian hospitals lack the capacity to manage snakebite cases effectively and that nearly all facilities experience difficulties in administering antivenom, the only treatment recognized by the World Health Organization for venomous bites. Such deficits in treatment capacity, emergency response, essential medicines, and clinical training are not anomalies; they are the predictable outcome of chronic systemic weakness.
Nigeria’s healthcare system is structured across primary, secondary, and tertiary levels. According to the latest facility registry data, there are roughly thirty-eight thousand six hundred forty-five operational health facilities nationwide, a figure that includes both public and private establishments, translating to approximately eleven facilities per one hundred thousand people in a population exceeding two hundred and twenty million. Primary care facilities account for nearly eighty-eight per cent of all facilities, secondary care roughly twelve per cent, and tertiary facilities less than one per cent.
On paper, the distribution seems extensive, but quantity does not equal quality or functionality. The majority of primary healthcare centers, which form the first line of defence, are unable to deliver essential services consistently due to shortages of trained personnel, drugs, water, power, and equipment. Only about twenty per cent of primary facilities are considered fully functional, leaving millions of Nigerians dependent on emergency care that is often delayed or unavailable.
Health outcomes are determined by human resources as much as infrastructure, yet Nigeria’s health workforce is severely strained. The doctor-to-population ratio remains well below the World Health Organization’s recommended threshold of one doctor per six hundred people, with practical estimates ranging from one doctor per four thousand to one per five thousand citizens, and some areas experiencing ratios as low as one per nine thousand eight hundred.
Nurses and midwives are similarly scarce and unevenly distributed, favoring urban centers over rural and peri-urban areas. Absenteeism and burnout are systemic risks exacerbated by poor remuneration, unsafe working conditions, and limited career progression. The migration of trained health professionals abroad not only represents a loss of public investment but reduces the system’s capacity to respond to emergencies, increasing the likelihood that predictable crises result in preventable deaths.
Funding is a primary driver of these gaps. Nigeria is a signatory to the 2001 Abuja Declaration, committing to allocate at least fifteen per cent of annual budgets to health, yet the highest allocation recorded in any year remains below six per cent. By comparison, global benchmarks suggest public health spending should constitute at least five per cent of GDP to achieve basic universal health coverage, while Nigeria currently allocates approximately half a per cent. Per capita health expenditure ranges between ten and fifteen US dollars annually, which is insufficient to ensure functional hospitals, reliable emergency response, or the availability of essential drugs and equipment.
The inadequacy of public funding shifts the burden to households. Out-of-pocket payments account for nearly seventy to seventy-five per cent of total health spending, meaning that patients and families finance care at the point of illness rather than through pooled systems. Less than ten per cent of Nigerians are covered by any functional health insurance, and coverage is largely limited to formal sector employment. As a result, families often delay care, ration treatment, or avoid facilities altogether until conditions deteriorate beyond recovery.
The human consequences of these systemic failures are evident in national health indicators. Nigeria continues to have one of the highest maternal mortality ratios in the world, exceeding eight hundred deaths per one hundred thousand live births, and accounts for approximately twenty per cent of global maternal deaths despite representing less than three per cent of the world population. Infant and under-five mortality remain high, with recent surveys showing roughly sixty-seven deaths per one thousand live births and one hundred and ten per one thousand respectively. Many of these deaths result not from rare or complex conditions but from the inability of the health system to provide timely, skilled intervention for preventable or manageable illnesses. Malaria, pneumonia, childbirth complications, and neonatal distress often escalate into fatalities that could have been avoided had emergency care been available, adequately staffed, and well-supplied.
Infrastructure alone does not solve the problem. Hospitals are renovated, equipment procured, and wards repainted, but functionality depends on staffing, reliable power, water, supply chains, and governance. Electricity supply is particularly critical, as hospitals depend on continuous power for monitoring, oxygen delivery, laboratory diagnostics, and refrigeration of vaccines and essential medicines. Yet many facilities rely on intermittent generators with uncertain fuel supply, leaving patients exposed to system failures that no renovation or new building can correct.
Primary healthcare centers, despite their numbers, are frequently unable to provide preventive and early intervention services, meaning that conditions that should be addressed at the community level escalate to secondary facilities that themselves are overstretched.
Accountability within the health system is diffuse. Budget allocations are announced, but utilization and outcomes are weakly monitored. Staffing requirements are often unmet, and enforcement is inconsistent. Failures rarely attract consequences proportional to their impact, leaving citizens, including vulnerable infants and young adults, to bear the cost. Hospitals are frequently evaluated on the wrong metrics, such as bed count or physical infrastructure, rather than whether care is actually delivered. Time-sensitive emergencies cannot wait for policy announcements or cosmetic compliance; delays and absenteeism in these circumstances are measured in lives lost.
Both my personal experience and the case of the young singer illustrate these realities. My daughter was taken to Suleja General Hospital where initial symptoms did not appear severe, yet she required urgent intervention. Medical review was delayed, oxygen was administered without a definitive diagnosis or treatment plan, and a requested transfer to another facility was not effected in time. In the singer’s case, urgent antivenom administration was critical to survival, yet the system’s gaps prevented timely care, and the result was fatal. These outcomes are not anomalies; they are predictable expressions of systemic failure.
Nigeria does not lack reform frameworks. Initiatives exist to revitalize primary healthcare, expand health insurance, and improve maternal and child health outcomes. Some interventions have produced measurable gains in targeted areas, but they remain uneven and insufficiently scaled, often undermined by governance failures and weak operational oversight. The result is a system that prioritizes form over function, presenting the appearance of readiness while leaving emergency response and routine care vulnerable to failure. The consequences are borne not by policy-makers or administrators, but by citizens whose lives hang in the balance.
The purpose of revisiting last week’s column is not to relive personal grief but to insist on institutional reflection. Every preventable death, whether of a child in a public hospital or a young adult succumbing to a snakebite or otherwise, represents a failure of policy, funding, and governance. Healthcare is not an area where delays, absenteeism, or cosmetic compliance can be absorbed without consequence. Systems either respond, or they fail. In Nigeria, the record shows repeated, predictable failures. Mortality data, budget analyses, facility assessments, and lived experience all converge to the same conclusion: when the health system is tested, it often cannot deliver.
The crisis is visible, documented, and persistent. Nigeria’s hospitals function intermittently, supply chains are fragile, essential medicines are inconsistently available, and health workers are overstretched. Until outcomes, rather than infrastructure announcements, become the primary measure of success, preventable deaths will continue.
Tragically, the cost is measured not only in statistics but in lives that could have been saved. My daughter’s loss was personal, and the death of Ifunanya Nwangene was public. Both expose the same reality: a healthcare system that cannot guarantee timely, competent response in emergencies is not merely underperforming; it is failing its most fundamental obligation.
The reality requires less rhetoric and more reform, less emphasis on appearances and more attention to function. Budget allocations must be credible and linked to measurable outcomes, staffing requirements must be enforced, essential medicines and equipment must be reliably supplied, and emergency systems must be consistently operational. Until these conditions are met, Nigeria will continue to produce tragic but predictable stories of lives lost to systemic weakness, and citizens will continue to confront a healthcare system that appears reassuring until it is tested at its most critical moments.

Nigeria, the Coup Question and the Burden of History, by Boniface Ihiasota
For Nigerians in the diaspora, the confirmation of a foiled coup attempt against the administration of President Bola Ahmed Tinubu is both disturbing and deeply unsettling. It is the kind of news that instantly revives memories many hoped had been permanently buried—years of interrupted democratic journeys, military decrees, suspended freedoms and national stagnation. That the military high command has now acknowledged that some officers are under investigation for alleged plotting only reinforces a painful truth: democracy must be constantly guarded, even decades after its restoration.
Nigeria’s long encounter with military rule gives special gravity to any suggestion of unconstitutional ambition within the armed forces. From afar, where Nigeria’s progress is often measured against global democratic benchmarks, the very word “coup” carries an ugly resonance. It recalls an era when power was seized, not earned; when institutions were weakened rather than strengthened; and when ordinary citizens bore the brunt of elite recklessness. Against this background, the assurance by Defence Headquarters that implicated officers will face trial under the Armed Forces Act is appropriate and necessary. In a constitutional democracy, there can be no justification for mutiny, armed insurrection or any conduct that undermines civilian authority.
However, the handling of information surrounding this incident leaves much to be desired. Weeks of denial and silence before official confirmation created a vacuum quickly filled by rumours, speculation and anxiety. For Nigerians abroad—already sensitive to how instability at home affects the country’s image, investment prospects and diplomatic credibility—this lack of clarity was troubling. Transparency is not merely a public relations tool; it is a democratic responsibility. Investigations must be rigorous, evidence-driven and insulated from political interference if public confidence is to be restored.
It is equally important to draw a firm line between legitimate political opposition and criminal conduct. Democracies function on debate, dissent and accountability. Public criticism of government policies, especially amid rising economic pressures, does not amount to subversion. The Tinubu administration must therefore avoid politicising the matter or using it to blur the distinction between lawful opposition and professional misconduct within the armed forces. To do otherwise would risk eroding democratic norms in the name of protecting them.
The broader continental climate makes the situation even more delicate. Across parts of Africa, democratic reversals have become alarmingly frequent. Military takeovers in Niger, Mali, Burkina Faso, Guinea and Chad—often justified by insecurity, economic hardship or governance failures—have reshaped the region’s political landscape. These developments explain why reports of a coup attempt in Nigeria last year triggered immediate concern. Nigeria is not just another country; it is a regional anchor. Any disruption to its democratic order would send shockwaves across West Africa and beyond.
From the diaspora perspective, a military intervention in Nigeria would represent a catastrophic setback. It would undo the gains of the past 26 years of uninterrupted civil rule and jeopardise the future of a country still striving to consolidate its democratic institutions. It would also complicate Nigeria’s international relationships, weaken investor confidence and further strain an already fragile economy. Above all, it would betray the expectations of millions of young Nigerians who have grown up under civilian government and demand better governance, not authoritarian detours.
The armed forces, therefore, must remain focused on their core constitutional duties. Nigeria is confronted by multiple security challenges: Boko Haram and ISWAP insurgencies, banditry, militancy and other forms of organised criminality. These threats require professionalism, discipline and unity—not political adventurism. Any internal distraction weakens the military’s capacity and emboldens non-state actors who thrive on instability.
Yet, responsibility does not rest with the military alone. History shows that while coups never offer lasting solutions, they often emerge in environments marked by economic distress, weak institutions and public disillusionment. From outside the country, where Nigerians observe governance systems that deliver basic services and social protection, the lesson is clear: leaders must be responsive and accountable. Addressing inflation, unemployment and poverty is not only an economic necessity; it is also a democratic imperative.
Equally important is the careful management of public communication. The military and the government must ensure that information relating to the alleged coup attempt is handled in a way that reassures citizens and investors alike. Alarmist narratives or vague statements risk portraying the state as fragile and insecure, which benefits neither democracy nor national cohesion.
Finally, the military high command must intensify efforts to shield its officers from civilian and political inducement. Coups rarely succeed without external encouragement. Officers must be constantly reminded of the grave consequences of unconstitutional actions and the primacy of national interest over personal ambition. At the same time, sustained funding, modern equipment and continuous training are essential to maintaining professionalism and morale within the ranks.

Muammar Gaddafi’s Son, Saif al-Islam, Reportedly Shot Dead in Libya
Saif al-Islam Gaddafi, son of Libya’s former leader, Col. Muammar Gaddafi, has reportedly been shot dead in circumstances that remain unclear, Libyan media sources said on Tuesday.
The death of the 53-year-old politician was confirmed by the head of his political team, according to the Libyan News Agency.
However, conflicting accounts have emerged over the circumstances surrounding his death.
His lawyer told the AFP news agency that Saif al-Islam was assassinated at his residence in the city of Zintan by a “four-man commando” unit.
The lawyer did not disclose who may have been responsible for the killing.
In a separate version of events, Saif al-Islam’s sister told Libyan television that he died near Libya’s border with Algeria.
Saif al-Islam Gaddafi was long regarded as the most powerful and feared figure in Libya after his father, who ruled the country from 1969 until he was ousted and killed during a popular uprising in 2011.
Born in 1972, Saif al-Islam played a prominent role in Libya’s rapprochement with Western nations from around 2000 until the collapse of the Gaddafi regime.
Despite holding no official government position, he wielded significant influence and led high-level negotiations on behalf of his father.
These efforts included talks that culminated in Libya abandoning its nuclear weapons programme, a move that led to the lifting of international sanctions and restored diplomatic ties with Western countries.
At the time, Saif al-Islam was widely portrayed as a reformist figure and the acceptable face of a changing Libya.
Following the fall of his father’s government, Saif al-Islam was accused of playing a key role in the violent repression of anti-government protests in 2011.
He was subsequently captured and detained by a militia in Zintan, where he spent nearly six years in custody.
The International Criminal Court sought his extradition to face charges of crimes against humanity related to the suppression of the uprising.
In 2015, a court in Tripoli sentenced him to death in absentia for his alleged role in the crackdown, although the ruling was rejected in eastern Libya.
He was released in 2017 by a militia in Tobruk under an amnesty law enacted by authorities in the east of the country.
Since the overthrow of Muammar Gaddafi, Libya has remained deeply divided, with rival governments and numerous armed groups controlling different parts of the country.
Although Saif al-Islam had repeatedly denied any ambition to succeed his father, insisting that power was “not a farm to inherit,” he re-emerged on the political scene in 2021 when he announced his intention to contest the presidency.
That election was later postponed indefinitely, prolonging Libya’s political uncertainty.
As of Tuesday, Libyan authorities had yet to issue an official statement clarifying the circumstances surrounding his reported death.



Diaspora Watch Vol. 81

Examining Nigeria’s Health System and Preventable Deaths, by Alabidun Shuaib AbdulRahman

Chief Chukwuma Johnbosco and the Making of a Purpose-Driven Leader

Pastor Jerry Eze Defends Miracles At UK Conference Amidst Criticism And Controversy

Diaspora Watch 20th Edition (October 14-20, 2024): Your Trusted Source for Global News and Insights

Tanzanian Man Reportedly Dies And Returns To Life Six Times



-
 Milestone4 days ago
Milestone4 days agoChief Chukwuma Johnbosco and the Making of a Purpose-Driven Leader
-

 Sports5 days ago
Sports5 days agoEx-Sri Lanka Star Jayasuriya Named in USA Squad for T20 World Cup
-

 News4 days ago
News4 days agoUS Sends Troops to Nigeria Over Rising Terror Threats
-

 Sports5 days ago
Sports5 days agoLens Edge Le Havre to Reclaim Ligue 1 Top Spot
-

 Sports5 days ago
Sports5 days agoJustin Rose Sets 36-Hole Record, Opens Four-Shot Lead at Torrey Pines
-

 News4 days ago
News4 days agoMuammar Gaddafi’s Son, Saif al-Islam, Reportedly Shot Dead in Libya